COVID-19 was declared a pandemic on March 11, 2020 by the World Health Organization.
That was the disease. Disinformation about COVID-19 reached pandemic proportions on March 12, 2020, as assessed by yours truly.
The COVID-19 pandemic has entered a strange phase, in which the risk of contracting the virus, driven by ever more contagious variants, continues to oscillate in waves. At the same time the risk of hospitalization and mortality from the virus has plummeted, thanks to near-miraculous achievements on the part of the biomedical research community in the form of rapidly developed vaccinations and effective treatments.
The COVID-19 disinformation pandemic, in contrast, continues to induce inflammation. Its etiology: the production of “alternative facts” and spurious statistics designed to appeal to those who subscribe to a good-guys/bad-guys worldview.
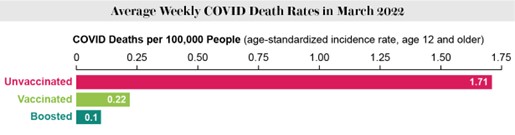
Example: The perception that being vaccinated doesn’t reduce COVID risks continues to be popular among a certain class of opinionator, armed with persuasive-looking but flawed statistics and positioned for high visibility in the popular media.
Revealing the flaws in their statistical reasoning depends on opinionators whose highest-visibility platforms are publications such as Scientific American – not where most citizens flock to develop their opinions. See the graph that follows (spoiler alert):
Nonetheless, for several reasons it’s time for organizations to revisit their COVID-19 policy. First and foremost, as of this writing and as noted above, the combination of currently available vaccines and clinically valid treatments – and yes, I mean Paxlovid, not quack therapeutics like Ivermectin – have made the consequences of an employee violating your COVID-19 policy less dire than they were in the early stages of the pandemic.
Second, as compared to 2020, the power dimension of the employer/employee relationship has shifted significantly in employees’ favor. As a practical matter, terminating an employee for violating policy probably harms the employer as much or more than the employee.
And third, the logic of targeting a policy to a single specific malady is increasingly tenuous.
The original purpose was to help create and maintain a safe work environment. But even before COVID-19, contagiously ill employees who came in to the office endangered their colleagues – not as severely as COVID in the pandemic’s early days, but of severe enough discomfort and debilitation to matter regardless of the specific malady.
Shortly before the first COVID-19 vaccines were released (late July, 2021) I suggested this COVID-19 policy:
All employees who:
- Enter our facilities …
- Enter a client’s facilities …
- Perform any of their responsibilities face-to-face with colleagues regardless of location …
- Enter our facilities …
- Enter a client’s facilities …
- Perform any of their responsibilities face-to-face with colleagues regardless of location …
… must be fully vaccinated. Refusal to comply with this policy can result in termination or reassignment to a position all of whose duties can be performed remotely. If the result is reassignment the company reserves the right to adjust compensation to make it commensurate with the new position’s pay structure.
This policy applies to all employees and contractors, other than those who can perform all work remotely.
What should change?
Mandating vaccination made sense when vaccines were effective against the most prevalent variants, and when the consequences of failing to comply concerned employees more. But that ship has sailed and there’s no point in pretending otherwise.
Also, as mentioned, broadening policy beyond COVID and only COVID would mean requiring employees to be fully vaccinated against everything that’s contagious and for which we have effective vaccines. This just won’t fly, regardless of the wisdom of being fully vaccinated.
Bob’s last word: Encouraging employees to be fully vaccinated is a matter of helping them stay healthy. Our arsenal of safe and effective vaccines is one of the blessings of modern medicine.
But mandating them? For better or worse the time for that has come and gone.
The alternative: Instead of mandating vaccination, requiring all contagiously ill employees to stay home makes all kinds of sense.
It makes all kinds of sense, that is, if their employer makes PTO policies more generous, so that ill employees no longer have an incentive to show up for work at the office, giving the gift that keeps on giving – a disease.
Bob’s sales pitch: Need help thinking through a situation you or your organization is facing? That’s what I do, and if you read KJR on a regular basis you should have a pretty good sense of the perspectives I bring to such things.
And you can get my help in increments as small as an hour.
Just let me know what you need.
Now showing on CIO.com’s CIO Survival Guide: “A CIO’s guide to guiding business change.” Because As CIOs re-think IT’s role in the enterprise, leading or facilitating business change is central to the conversation. Here’s one way IT can and should regain center stage.
Hi Bob,
Employees don’t always know if they are contagiously ill with COVID. Fact: vaccines reduce the number and severity of infections. A vaccinated person is less risky to close contacts than is an unvaccinated person.
True, vaccines don’t prevent all infections, transmissions, or deaths. They merely (significantly!) reduce risk. Similarly, brakes don’t prevent all traffic accidents, fatal or otherwise, but we still want every vehicle on the road to have well-functioning brakes.
Hospitals, congregate living facilities, and correctional facilities are all examples where vaccine mandates still can prevent a lot of disease and death. So, too, do vaccine mandates make a lot of sense for staff who go into customers’ homes, such as appliance technicians, in-home salespeople, and firefighters in a paramedic role.
Want to stay unvaccinated? You are misinformed or you prefer to take unnecessary risks, but OK. Then chose or adjust your career or job assignment so that you can stay away from the rest of us. Don’t put others at undue risk. And if it’s that you don’t trust vaccines or believe it’s a government (or Bill Gates or George Soros or Woke Left) conspiracy to control you, then, yes, that risk is undue.
You’re right, and I’ll amplify the point: With both COVID-19 and many other contagious diseases, victims may be infectious but asymptomatic for a period of time. My recommendation this week is a matter of not allowing perfect to be the enemy of good.
Even with professions for which infected workers might endanger large numbers of people around them, the line is increasingly hard to draw: Someone working in a modern call center with tiny cubicles and high densities endangers hundreds of fellow cube farmers.
Given COVID’s declining mortality it’s harder to justify mandates.
And we’ve seen how mandates have been received. At this stage of the game, better public information campaigns would, I think, be more effective.
But you aren’t wrong, either. More important than my specific recommendation is that we’re reaching a stage in which it’s time to re-think.
A whole lot of people have now had Covid. What is your assessment of antibodies/protection in people that have had Covid, compared to vaccine?
My assessment? I’m not qualified to make an assessment. From what I’ve read, it appears researchers have concluded that vaccines are more effective than natural immunity. Johns Hopkins has a nice write-up on the subject, but it’s old (November of last year): https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/covid-natural-immunity-what-you-need-to-know .
I haven’t yet read any updates that compare natural and vaccine immunity for the new Omicron strains. I suspect that for them, natural immunity is better, and will be until new vaccines tailored to the new variants become available.
“Shortly before the first COVID-19 vaccines were released (late July, 2021) I suggested this COVID-19 policy…”
The timing is off here. Better to rephrase that as “Shortly after COVID-19 vaccines began to be generally available (i.e. in late July, 2021)”.
My father, 91 years old and living in an Assisted Living Facility, received his first dose of Moderna vaccine on New Year’s Eve — December 31, 2020. This was part of a special early-access program specifically for seniors in group living arrangements.
I myself received my one-and-only dose of Janssen vaccine in April, 2021. This was the absolute earliest date I could get one, after trying for weeks to get an appointment via websites. The mainstream advice at the time, was: if you are lucky enough to get an opportunity to get a vaccine, TAKE IT, no matter which vaccine it is; don’t pass up an opportunity to get a vaccine, thinking that you want to wait for a different vaccine, because you can get infected, sick, and die, while you’re waiting. I thought that was good advice at the time, and I still do.
Later, vaccine appointments became more easily obtainable, and then after that, vaccines became available in pharmacies everywhere to walk-ins without a pre-arranged appointment.
A policy of “vaccines are MANDATORY for employees (unless specific exceptions)” is nonsensical, and even perverse, when vaccines ARE NOT ACTUALLY OBTAINABLE by employees, i.e. “before… vaccines were released”. But that same policy is reasonable, and justifiable, AFTER vaccines begin to be generally available.
So, give yourself proper credit! You did NOT recommend a policy that was nonsensical, and even perverse, at the time you recommended it!
– – – – –
On a different topic related to IT and Covid.. There’s the whole debacle about how vaccine appointments were offered to the public via websites. (Separately from vaccine appointments offered by healthcare providers to their already-current patients.)
The State of New Mexico did a superb job here: ALL publicly-available vaccine appointments were offered though the state government’s website; a resident of the state could register at that ONE website to be notified of ALL publicly-available opportunities for vaccine appointments in the state, and deliberately NONE were available on any other website, therefore there was NO NEED to repeatedly search multiple websites in a futile hope for an appointment to suddenly appear at one of them, and NO NEED to camp out for hours on websites pressing Refresh repeatedly hoping for an appointment to suddenly appear. Just register ONCE, at ONE website, and wait for an email notification to show up; there is NO NEED to do anything else, because nothing else will do any good.
One touch I admired: carefully crafted reassuring words and phrases that were repeated, word-for-word, in multiple places in the New Mexico state government’s website, for example: “If you have to cancel a vaccine appointment, DO NOT WORRY; this will NOT be your only opportunity to get a vaccine; you will be notified of future opportunities to get a vaccine.”
It’s hard to get go data on asymptomatic covid (those that never show symptoms of any kind during the course of their infection) because: testing and tracking of those with no symptoms happens far less frequently than those infected persons who eventually have symptoms.
So, I took a look at a couple of recent studies:
“A total of 28 studies that satisfied the eligibility criteria were included in this systematic review and meta-analysis…
In conclusion, one-fourth of SARS-CoV-2 infections are remained asymptomatic throughout the course infection.” .(https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0249090)
And,
“In conclusion, this study demonstrates that asymptomatic patients have higher SARSCoV-2 viral loads than symptomatic patients and unlike in the few study in the literature, a significant decrease in viral load of nasopharyngeal/oropharyngeal samples was observed with increasing disease severity. Factors associated with poor prognosis are found to be significantly correlated with low viral load.” https://link.springer.com/article/10.1007/s15010-020-01548-8
If a person wants to risk their own life, so be it. The facts speak for themselves. But mandates are to protect other workers, especially those in high risk groups.
You say, “…Instead of mandating vaccination, requiring all contagiously ill employees to stay home makes all kinds of sense.”
The problem with the above approach is that the most contagious employees can’t know that they are contagious until they are tested because they have no symptoms.
Vaccine mandates for covid is what the science dictates, though it is challenging to implement in our current “choose your own facts” culture that a minority clings to.
Besides, vaccines work well to keep you out of the hospital or dead, even for BA.4 and BA.5. I understand that UCSF experts say even getting covid will only protect you for about 4 weeks against the same variant.
We have to change our behavior before this virus evolves into something that wipes us out.
A whole lot of people have had Covid and claim that gives them antibodies/protection. What is your assessment of prior infection as compared to vaccine?
This was true until the omicron variants. I checked out 6 recent papers, but this one seemed sum things up best:
“Different from other variants of concern (VOCs) of SARS-CoV-2, the Omicron variant and its sublineages exhibit increased transmissibility and immune escape from neutralizing antibodies generated through previous infection or vaccination, and have caused numerous re-infections and breakthrough infections.”
“The most important feature of Omicron strains is their remarkable ability to evade immunity in convalescent COVID-19 patients and vaccinees. 19 Numerous studies have reported that BA.1 and BA.2 could effectively reinfect convalescent COVID-19 patients. Moreover, BA.2.12.1, BA.4 and BA.5 bearing the lineage-speci?c L452Q/R mutation could cause significant humoral immunity escape. Previous study has shown that L452R is also related to cellular immunity evasion. Currently, several studies reported that BA.2.12.1, BA.4 and BA.5 could further escape from the immunity induced by BA.1 or BA.2 infections, resulting in numerous re-infections in many countries.
In terms of vaccine escape, current research shows that these approved vaccines, even with routine dosing, still failed to prevent the outbreak of Omicron variants.”
https://www.nature.com/articles/s41392-022-01105-9.pdf
In plan English, the omicron variant, especially, but not limited to, BA.4 and BA.5
– Can reproduce faster
– Can avoid our white blood cells better
– Have more effective spike (docking) proteins
All result in reinfection, even of the same variant in those who have recovered from a covid infection or been vaccinated.
But, vaccinations, with boostings are still good at keeping you out of the hospital and out of the morgue.
Note that,
“For the week ending July 16, the majority of cases in the U.S. came from an Omicron sub-variant with 77.9% from BA.5, 12.8% from BA.4, 8.6% from BA.2.12.1, and 0.6% caused by BA.2.”
https://disasterphilanthropy.org/disasters/covid-19-coronavirus/?gclid=EAIaIQobChMI4qTX3Yqb-QIVvj2tBh1WJQb_EAAYASAAEgJvyPD_BwE
While these are early studies on omicron, I think they speak for themselves.
Hi Bob,
Fear is a mind killer. It opens one to being manipulated into doing and accepting things which may otherwise seem unethical or immoral. It does not allow clarity of though but rather allows for control. Judging by your column and reader comments, your government and media have done an absolutely fantastic job of instilling that fear in you.
Referring to Ivermectin, one of the safest drugs around with billions of doses being administered over the decades, whose creators received a Nobel prize for its creation, as “quack therapeutics” displays ignorance. Wanting to force mandates onto fellow humans, coerce them into taking medications against their own judgement again shows ignorance of Nuremberg code. Seems to me that if the Tuskegee experiment was done today, you and the commentors above would be cheering the government along. Or perhaps it is the fear doing that to you…?
You should expand your bubble, the world is bigger than just America. Out here is deepest, darkest Africa we have the lowest rates of COVID-vaccine uptake but yet the lowest rates of infections and deaths. Meanwhile in America, Europe and elsewhere with the highest rates of COVID-vaccinations, one finds the highest rates of infections with waves upon waves. Weird, huh?
Don’t worry though, you have monkeypox to look forward to and an unending stream of vaccines that accompany them, to be added to the already bulging schedule in the US – is it up to 50 vaccines before you’re 21…? When the monkeypox vaccine arrives, don’t forget to rush out and get your quintuple dose, no matter how experimental, along with your nth booster for covid. Don’t question. Just succumb to the fear.
Cheers.
Invermectin is an approved treatment for a number of intestinal parasites. SARS-CoV-2 isn’t an intestinal parasite, and the clinical evidence doesn’t support its use as a COVID-19 therapeutic (https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2789362 ).
A point we agree on: Fear makes people stupid. A related point: Anger has the same effect.
Yes, all those angry masked people who were manically shouting at their fellow human beings whose masks were under their nose or God forbid, did not wear any… deriding them as evil and killers. Weird how when mask mandates were dropped, no one who did not wear a mask walked up to those who still chose to wear one and started shouting at them to take it off.
About Ivermectin, I could show you studies showing the opposite but this is not a Let’s-See-Who-Has-The-Most-Articles swinging contest. You could check out what doctors on the ground have to say, at least those who have escaped being deplatformed or demonised for daring to voice an alternate opinion. Maybe, if you want to expand your bubble, start with one of the most published medical professionals, Dr Peter McCullough or Dr Pierre Kory.
I would also like to point out the corruption of science that has occurred over the past decades where many scientists/professors/researchers would not necessarily be true to what evidence presents but rather to what their employers or grantors would like it to be. To believe otherwise is to be naive – https://unherd.com/2021/05/how-science-has-been-corrupted/ Case in point, the Director-General of the WHO recently overrode his advisory panel who voted against the decision, to declare that he decided monkeypox was a global health emergency. Hmmm… billions starving, millions traumatised through isolation/depression, children physical/emotional/mental development stunted through policies that harmed them, 2 years of governments killing their economies – no, those are not as important… a few thousand cases of monkeypox are exponentially more existential threat to us. Or your FDA who no longer will require human trials for upcoming covid-vaccines, Pharma will submit evidence of animal testing and previous. Does not matter if it was for a different variant. Now, I would call these examples “quack therapeutics” but that’s just me. Don’t question. Just accept.
On the Covid disinformation issue, we can agree that we have been barraged by all sorts of information, some of it quite wrong. But even information from trusted sources, public health officials who spoke confidently, were often wrong. Much has related to efforts at censorship via the Trusted News Initiative (TNI) as created by health officials following guidance of Event 201 simulation. That effort actually enforced certain concepts like regional lock-downs that data now prove as not particularly effective in slowing the spread; anybody speaking out about the economic risk of that strategy was cancelled.
Fear is quite powerful and the counter to that is public debate. Once data arrived that showed 1000X IFR differences, we needed nuanced approaches to public risk. Because of the TNI the public discourse was not allowed and people often began to mistrust officials leading to “alternate” sources. As it turns out reporters like Alex Berenson were, in fact, accurate in reported contrary peer-reviewed data but was kicked (now restored) from Twitter.
We are still in the learning phase of this pandemic and discovering data from early days along with policy is no longer as useful for the circulating virus variant. Management must overcome inertia and change as needed. We can hope public health officials can admit error as data informs.
Just my perspective: Someone isn’t in error when they’re presenting the best available information. They’re in error when they ignore the best available information.
If the best available information turns out to be wrong, well, that’s how science works.
Error is what happens when someone just makes something up and presents it as fact.